In a continuation of the service done on Mental Health Awareness Week last October, this one focuses more on dealing with your own mental illness stigma and understanding mental health for anyone.
Speaker & Worship Leader:- Barbara Thomborson
Read below, or download the PDF
The personality disorder in you
Last October I led a service on the United Nations’ Mental Health Awareness Week. Many who were present at that service commented favourably on new understandings of mental ‘illness’ and mental health and asked for more. Today’s service is that follow-up.
As someone with lived experience of a mental health diagnosis, I have used mental health services for decades. Before I accidentally retired, I was an advisor with Auckland DHB’s mental health services.
Last year’s Mental Health Awareness Week focused a lot on stigma against those with mental ‘illness’. Instead of mental ‘illness’, I strongly prefer the term different mental condition. Precolonial Maori considered those we would call mentally ill as different. I choose to use that term in this sermon.
By understanding your own mental health, you can lessen your stigma about mental illness or mental conditions that differ from what we call healthy or normal. Mental health quality is on a continuum in two ways – within a person and relative for each person in society. Our mental health moves fluidly but usually not rapidly along this continuum. This fluidity enables us to understand our personal growth and to connect with others on a deep level.
Last October, we considered the progression of how anyone could developing auditory hallucinations, also known as hearing voices. That exercise helped us understand how anyone might develop auditory hallucinations. With that understanding we could sympathise with those
who hear voices that disrupt their lives. This slide describes that progression.
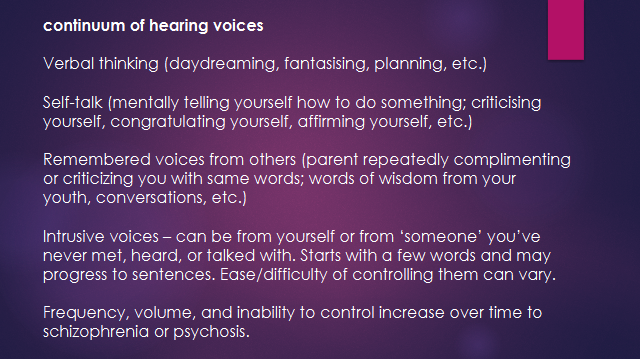
- Verbal thinking (daydreaming, fantasising, planning, etc.)
- Self-talk (mentally telling yourself how to do something; criticising yourself, congratulating yourself, affirming yourself, etc.)
- Remembered voices from others (parent repeatedly complimen-ting or criticizing you with same words; words of wisdom from your youth, conversations, etc.)
- Intrusive voices – can be from yourself or from ‘someone’ you’ve never met, heard, or talked with. Starts with a few words and may progress to sentences. Ease/difficulty of controlling them can vary.
- Frequency, volume, and inability to control increase over time to schizophrenia or psychosis.
Today I’m attempting a more complex comparison for you to understand: personality disorders. I hope by the end of this part of the service you can see how someone might develop a Personality disorder or even have one yourself. American spiritual philosopher, psychologist, and writer Ram Dass said it this way: “… you’ve got to understand that your ability to see the soul and subtlety inside of another person is in part dependent on your ability to acknowledge it in yourself”. It’s easier to see and understand it in someone else if you have seen it in yourself. So let’s try to acknowledge that part in each of us that could evolve into a personality disorder.
The term “personality disorder” may imply that there is something not-quite-right about someone’s personality – that it is disordered, broken or wrong, or that they are somehow a bad person, even scary. But that is not what the words are intended to mean. These terms merely help clinicians group a set of typical features for people with problematic aspects of their personality. These aspects can cause serious problems for someone and be challenging for those around them. Psychologists recognise 10 prevalent personality disorders, the most common of which are borderline PD and antisocial PD.
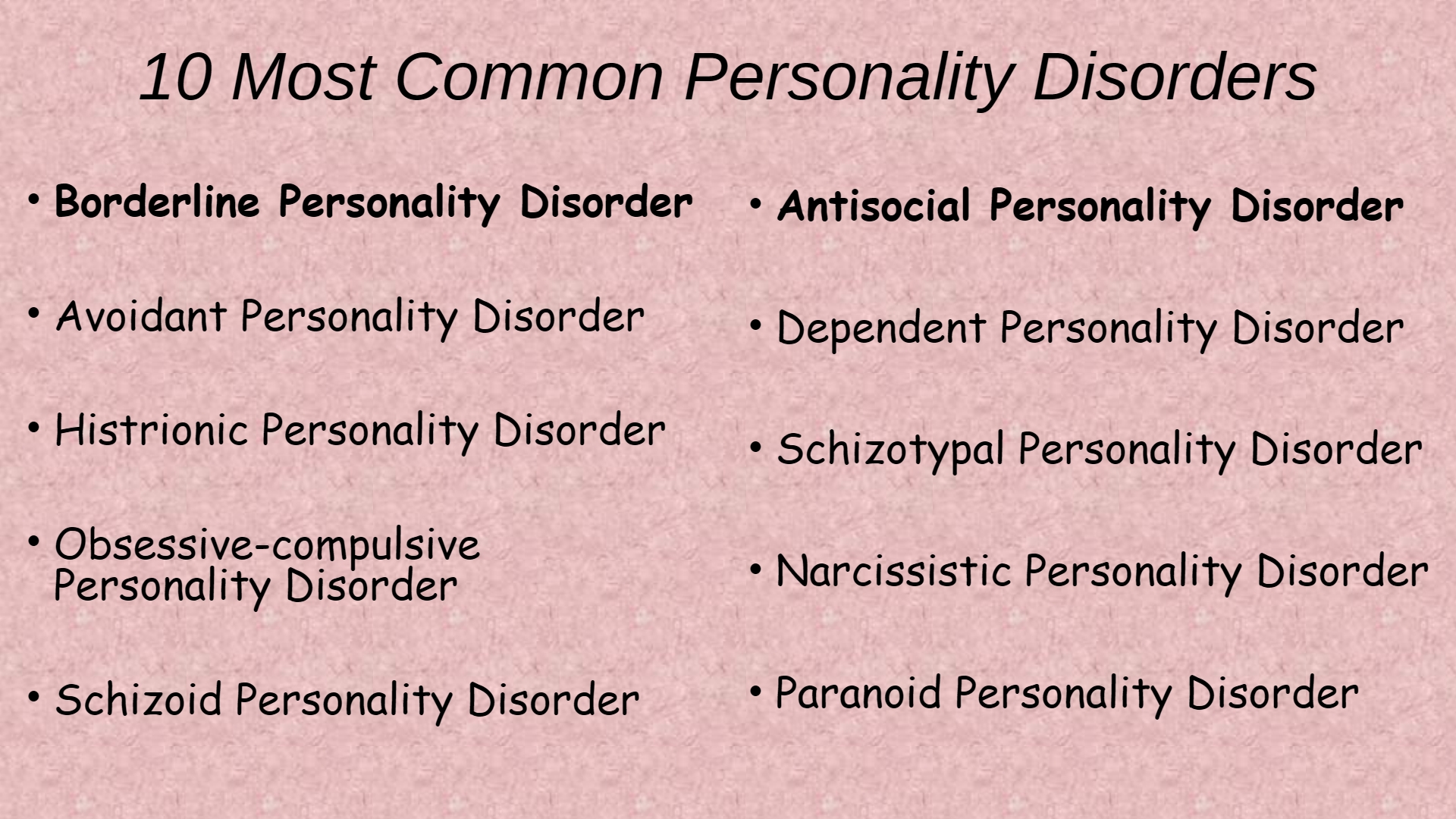
10 Most Common Personality Disorders
Borderline Personality Disorder
Avoidant Personality Disorder
Histrionic Personality Disorder
Obsessive-compulsive Personality Disorder
Schizoid Personality Disorder
Antisocial Personality Disorder
Dependent Personality Disorder
Schizotypal Personality Disorder
Narcissistic Personality Disorder
Paranoid Personality Disorder
These are the 10 most common personality disorders. All of them carry a load of stigma, especially Borderline and Antisocial. They are in bold because they are the most commonly diagnosed.
Someone with lived experience of a PD advised that we “Look at [personality disorder] behaviours as on a spectrum of human behaviour. We all have times of some of these features, but for some of us, they end up clustered together, making life more difficult. So much of life is bound up in relationships, and being able to ‘people’ is important to well-being”.
Within this list, let’s consider aspects of personality disorders in which you may recognise as some of your own traits.
What does it mean to have a personality disorder? People with personality disorders often have a hard time understanding emotions and tolerating distress. Regulating their emotions is challenging, sometimes impossible depending on the amount of chronic stress or trauma in their past. Have not all of us here had trouble understanding emotions, your own and others’? Have you ever tolerated distress well or handled it really unwell? And about managing your emotions, have you never had an outburst of anger that lasted longer than you wanted? Can you think of a time when your emotions were quite out of line and you could not get on top of them? As well, those with personality disorder act impulsively. Acting impulsively can be confused with acting spontaneously – they are closely related, no? Impulsivity, however, comes with maladaptive behaviours and disorders such as drug abuse, gambling, or obesity; impulsivity can lead to addictions. That begs the question, have you ever thought that you may have an addiction? Consider our alcohol culture and ask yourself how often you rely on a glass or two of wine or beer to unwind after work. Addictions are a common trait for diagnosing some personality disorders.
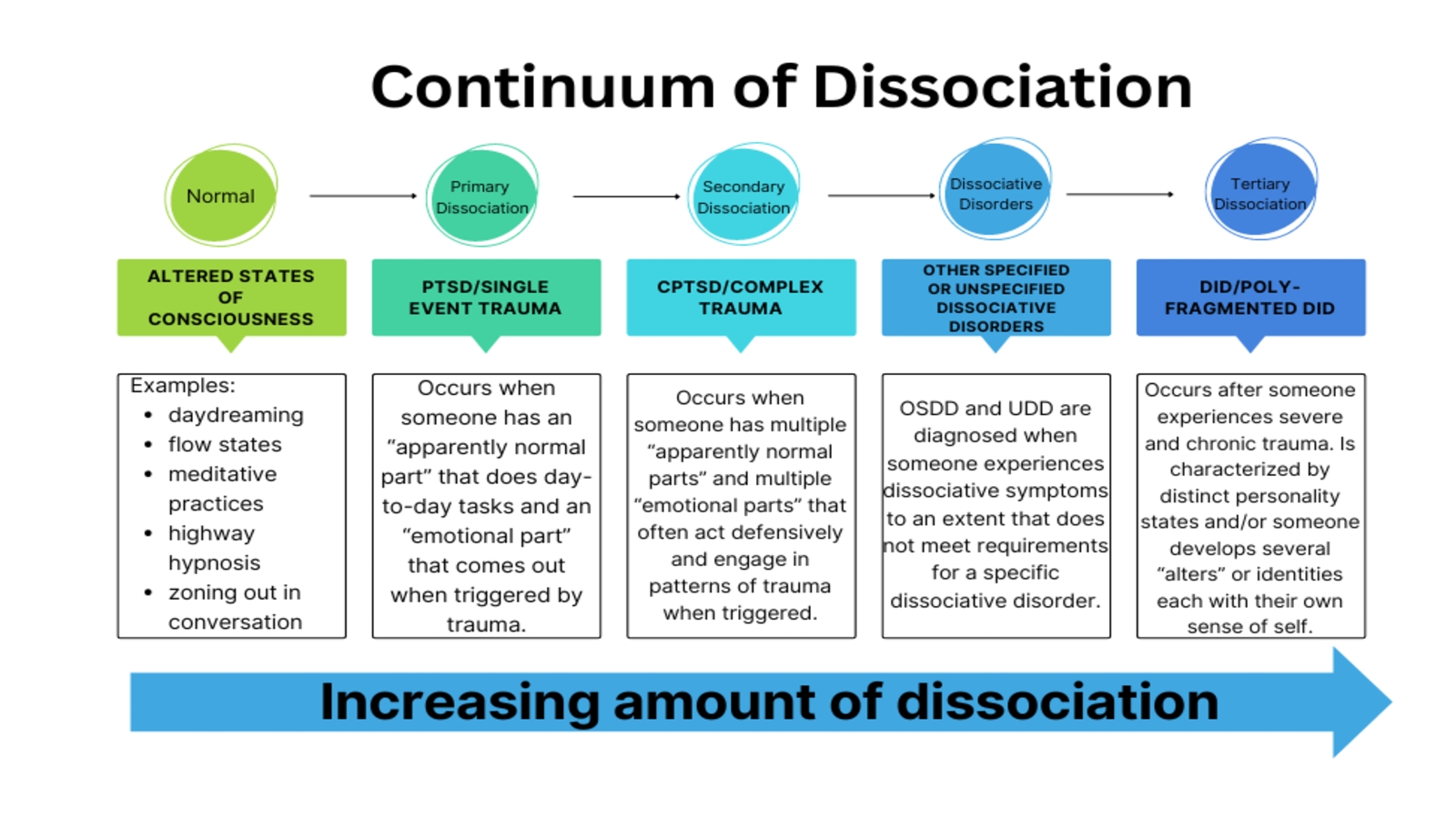
Another experience in some people is dissociation. In fact, those who experience a lot of dissociation have their own named PDs. Dissociation is a mental process involving a disconnection between a person’s thoughts, memories, feelings, actions, or sense of identity. It is a subtype of psychosis involving a disconnect with reality but usually not as intense as psychosis. Dissociation is part of mood disorders. It’s like seriously zoning out. Amnesia is an advanced form of dissociation.
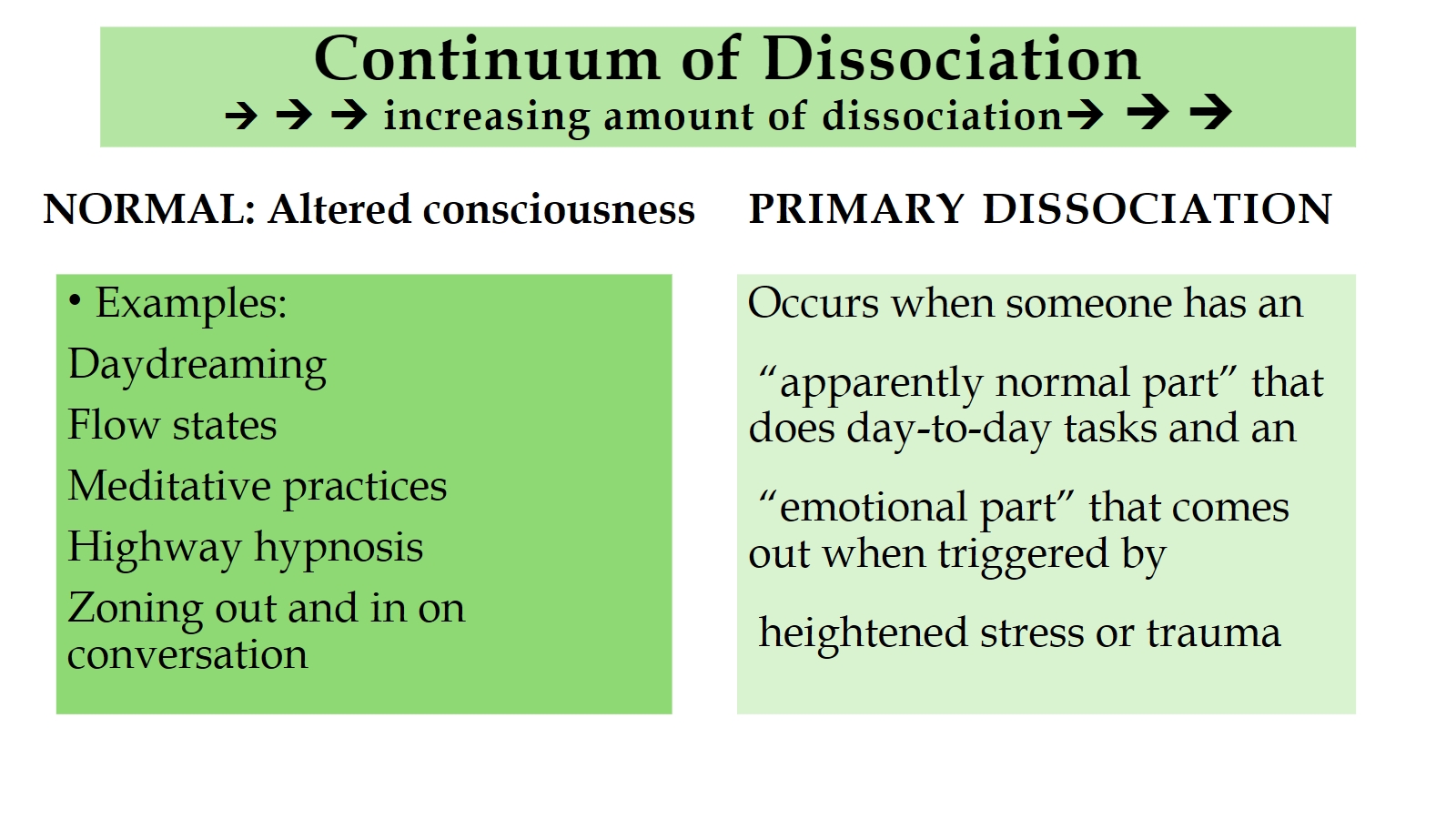
>>>increasing amount of dissociation>>>
NORMAL: Altered consciousness
Examples:
Daydreaming
Flow states
Meditative practices
Highway hypnosis
Zoning out and in on conversation
PRIMARY DISSOCIATION
Occurs when someone has an
“apparently normal part” that does day-to-day tasks and an
“emotional part” that comes out when triggered by
heightened stress or trauma
Look at the first, normal, stage. Who has NOT experienced all of these – daydreaming; flow states; meditative practices; highway hypnosis; zoning out and in on conversation? This personal acknowledgement enables us to relate personally with psychological dissociation. As an example, while filling up my car at a petrol station, I once forgot to put the nozzle back and almost drove off. That was a rude wake-up for me; given that I was under a lot of stress in those days, I was probably in stage two dissociation.
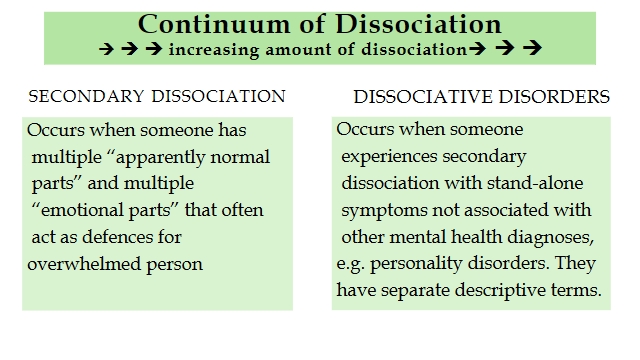
>>> increasing amount of dissociation >>>
SECONDARY DISSOCIATION
Occurs when someone has multiple “apparently normal parts” and multiple “emotional parts” that often act as defences for overwhelmed person
DISSOCIATIVE DISORDERS
Occurs when someone experiences secondary dissociation with stand-alone symptoms not associated with other mental health diagnoses, e.g. personality disorders. They have separate descriptive terms.
I call these two types of dissociation the debilitating stages. People who experience them need professional help.
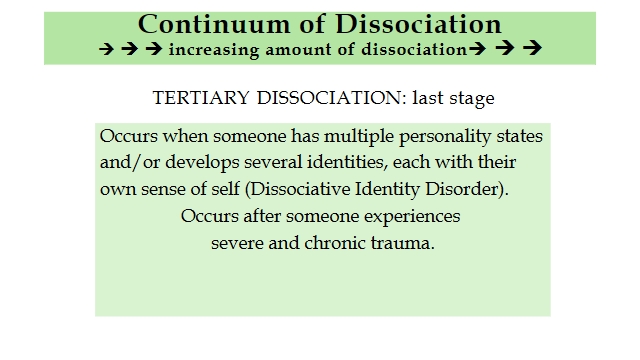
>>> increasing amount of dissociation >>>
TERTIARY DISSOCIATION: last stage
Occurs when someone has multiple personality states and/or develops several identities, each with their own sense of self (Dissociative Identity Disorder). Occurs after someone experiences severe and chronic trauma.
Tertiary, last stage, dissociation often comes and goes but is usually just under the surface of consciousness, like underlying dissociation. Triggers include reminders of past trauma, both subtle and obvious.
Again, I’m sure all of us can relate to this occasional disconnection with our usual reality, so we can understand how this disconnection could progress to something harmful or dangerous.
Many regular people have a predisposition towards a PD; only when the right stresses or trauma occur in their lives does the PD manifest. It is possible that you may have a personality disorder and not know it. For example, many with BPD do not know they had it until a lot of stresses and/or a traumatic experience brought it out, and they had big problems in their daily lives. I know someone with BPD who did not get their diagnosis until they were 58. They excelled in employment and at university, were President of their university’s student congress, and earned the highest award for service to the student body for that year. They went on to teach at university. Psychologists call this type “quiet” BPD. Such people appear composed, successful, and stable on the surface—often holding demanding jobs and maintaining active social lives, just like you—while internally battling severe emotional turmoil, intense fear of abandonment, and deep self-loathing. Yet their lives look ‘normal’; many with PDs have successful careers and hold positions of leadership and great responsibility. In fact, those in careers as professors or medical doctors make up most of those diagnosed with narcissistic PD. So, I advise you not to assume everyone who is successful and seems happy has good mental health. I cannot overstress, we are all on a continuum of mental health, each with our own mental health conditions.
I hope this foray into relating to those with PDs has expanded your understanding and compassion for those who suffer and struggle with PDs. I hope you can see yourself in them and see them in you, as well as reducing any stigma towards those with PDs. It’s an important aspect of our interconnected web of life, in this case, our social lives. And I hope you can count yourself blessed that you don’t have an impairing PD.
Happify yourself!
Besides developing your understanding and compassion for those with PDs, last year’s Mental Health Awareness week also focused on personal mental health. Let’s consider happiness as an aspect of good mental health. I like this definition of happiness: an enduring state of well-being involving satisfaction in the pleasant, good, and meaningful aspects of life. A happy life has a sense of meaning and deep contentment. Let’s not confuse happiness with feeling really good or bouncing from one joy to the next.
Research into the psychology of happiness started in the 1990’s but it’s based on historical and modern philosophies. When a reporter asked Freud what we need for happiness, he replied: two things – satisfying relationships and satisfying occupations. Modern happiness researchers took Freud’s analysis of happiness and added a third – hope. However, some happiness experts say a sense of purpose is more important than hope.
Happiness researchers have created a whole new area of psychology. Have you ever considered that you can grow happiness in yourself? I found the notion of growing happiness, like a plant or something, a radical idea until I started researching it. The biggest factor in growing personal happiness centres on choices you make. They’re not just the big life choices like your job, your partner (or not to partner), where you live, to have children or not, etc. Those choices carry the big stakes for personal happiness, of course. But for that enduring sense of well-being and contentment, essentially regardless of what life throws at you, your small choices count as much. These are your everyday choices, even sometimes of minor things.
Slide 7: EVERYDAY CHOICES THAT AFFECT YOUR HAPPINESS
- choices about relationships,
- choices about your health,
- choices about physical aspects of your life outside of health,
- choices about managing stresses,
- choices about managing your emotions,
- choices about your spiritual life.
They include choices about relationships, choices about your health, choices about physical aspects of your life outside of health, choices about managing stresses, choices about managing your emotions, and choices about your spiritual life.
Research in positive psychology, including the ‘science’ of happiness, is rife with traits of happy people. From my research into happiness, I’ve culled this list of traits that lead to enduring contentment:
SLIDE 8: TRAITS OF HAPPY PEOPLE: THEY
- live in the present and do not get hung up on the past.
- see opportunities instead of problems.
- find happiness in the small things and make a habit of enjoying common pleasures.
- value internal sources of happiness more than materialistic things.
- are grateful and count their blessings.
- don’t get stuck when awful things befall them.
- give and share generously.
- have satisfying social lives.
- are curious about new and old things.
- make careful choices.
1. Happy people live in the present andare not too hung up in the past, nor worry too much about the future.
2. Happy people see opportunities instead of problems: They accept that life has hard challenges, even tragedy, and understand that within difficulty lies opportunity.
3. Happy people find happiness in the small things and make a habit of enjoying common pleasures likesun on their face as they walk outside, spending time with a good friend, the smell of newly cut grass, etc.
4. Happy peoplevalue internal sources of happiness over materialistic things.Experiences, relationships, and small things in life bring them more joy than materialistic things. This value is essential for spiritual development.
5. Happy people are grateful and count their blessings.They appreciate what they already have, instead of always wishing for more and more and more, never getting fully satisfied.
6. Happy people don’t get stuck when awful things befall them. They spend little time complaining and feeling sorry for themselves – they know when it’s time to move on.
7. Happy people give and share generously. Unhappy people are often greedy, selfish and not very willing to share, while happier people are generous to others with their time, money, and resources.
8. Happy people have satisfying social lives. Humans are among the most social animals; isolation for us often leads to depression.
9. Happy people are curious about new and old things. They continue to add to what they know about meaningful things in their life and embrace learning about new things.
10. They make careful choices. The everyday choices contribute more to growing happiness than the big life choices. Everyday choices contribute to making habits of the previous 9 happiness traits.
For more about the ‘science’ of positive psychology, the website happify.com has extensive information that’s easily accessible. They’ve been online for almost 15 years with a team that provides a practical array of topics, discussion forums, games, and other activities. Again, I recommend happify.com for practical, mostly free information on how to live happily.
I end this talk with a Buddhist well-wish: May you be well, may you be at peace, and may you be happy.
Meditation / Conversation starter
- How has this talk made you think differently about personality disorders?
- Which of the personality disorder traits did you find most in yourself?
- What do you think of the idea that you can grow happiness in yourself?
Links
- Opening Words:- are from “Come into this circle of community. Come into this sacred space.” by Andrew Pakula
- Chalice Lighting:- “First Principle Chalice Lighting” by Florence Caplow
- Closing Words:- “Mindful of our highest aspirations” by Rebecca A Edmiston-Lange